
This has been my fourth year teaching the Arts and Science of Clinical Medicine I (ASCMI) at the Mississauga of Medicine. The course sets out a general curriculum we follow every Friday morning for four hours with a group of six students. Students learn basic history and physical exam skills. Although the curriculum is highly structured my group has always loosely following the curriculum by also dealing the hidden curriculum. Beyond clinical skills we frequently discuss the process of becoming a physician, school stress or any other topic brought on by my learners. I have done my best to be flexible to my learner’s needs running an unstructured group and responding to individual learners and bringing my own clinical experiences and stories to the learning process. My modus operandi this year was quite the same.
December of this year I left for an extended trip lasting about seven weeks. When I returned I received anonymized summarized feedback from my students. Much too my surprise the feedback was split with half the group rating my skills highly and half moderate-low. Furthermore while I was absent many of my students had communicated to my colleague that our group was disorganized, not meeting their learning needs nor course requirements. Given the amount of positive feedback I had informally received since the beginning of the academic year I found this disorienting.
To help provide some context I had discussions with former students who were now in their second and third years in their studies. They clearly stated under my supervision when they were taking ASCMI, they were grateful with approach we used to learn how to direct an interview from chief complaint to broad differential to narrowed list of likely diagnoses. Furthermore they felt they could incorporate knowledge from future courses into this approach. Lastly they were grateful for the multiple tangential conversations covering what it means to be a physician and moral and ethical challenges presented in medical school and how these challenges change over the years of medical education and continue into practice. However, all my former students had also had come to accept that we rarely covered all the components in the course manual and definitely did not cover the fine minutiae in any detail. When they compared the education they received by their colleagues at our sister hospital, we spent much more time on the art while their peers spent time on the science. Nonetheless they stated they preferred our methodology as they felt they could learn the minutiae independently and always felt comfortable bringing up points from the course manual that were confusing. They enjoyed spending time on the broader aspects of medicine that were not covered strictly in the course.
After getting perspective from prior students I gathered my current students to look for feedback and direction for how our group should function. I left this discussion bewildered. The views expressed from my learners ranged from:
- Our sessions lack any structure, are not covering the course curriculum, the group dynamic needs to be fundamentally shifted, we need to be constantly questioned and grilled to ensure we are learning our course objectives
- We can make a few moderate changes to improve our learning
- Why are we having this discussion? We currently have a safe learning environment that supports our learning
From my perspective I was happy to teach the curriculum in whatever manner my learners desired – either highly structure like my colleagues at my sister hospital or using my typical methods. I just needed clear directions on what to do. The variety of views expressed and lack of consensus arrived by my students lead me to believe that the power imbalance my presence created an impediment to my learners arriving at a common consensus. This conclusion lead me to instruct my group to develop a group charter independently of me to be reviewed at our next session. Removing myself from the conversation allowed my learners the safety to arrive at the below plan without fear that individual views would be lead to consequences to their evaluations.
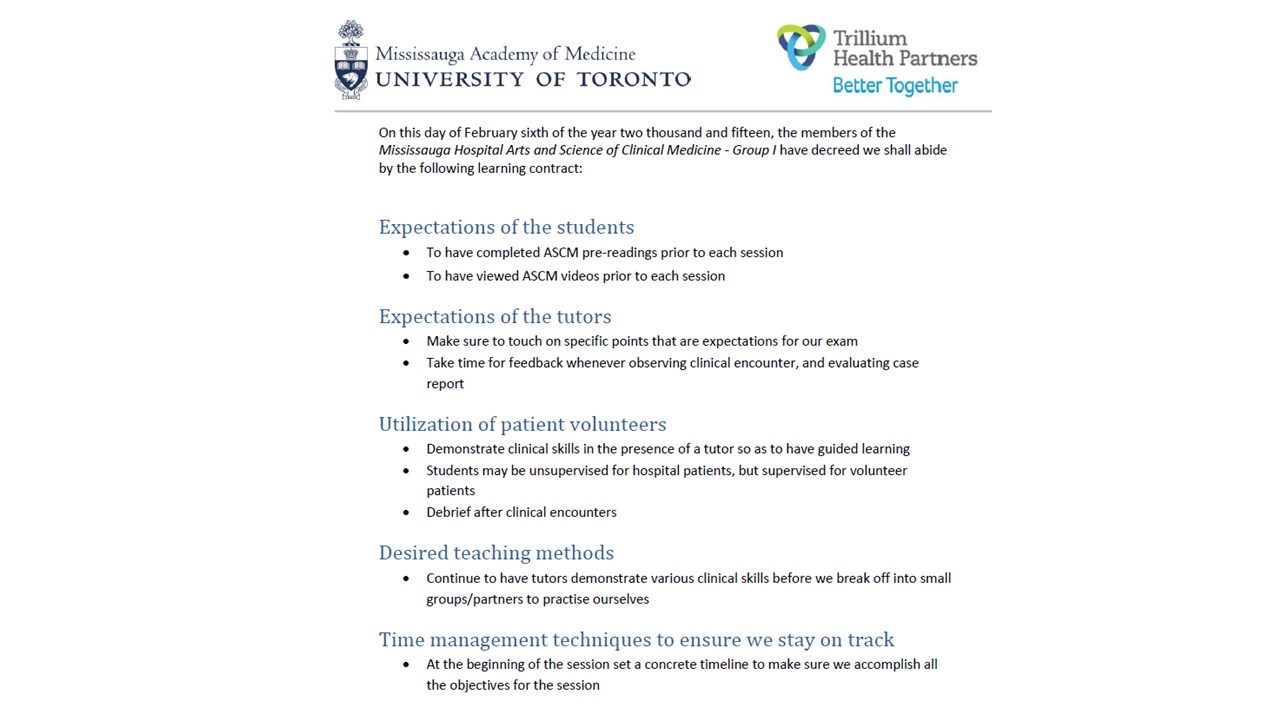
Even though this charter may not seem complex it outlines how the group should function and more importantly I believe the process of my learners coming to a consensus about what they want from this course. Now we are more focused on the core curriculum but have the freedom to discuss other matters – but often on a one to one basis.
This experience has taught me to appreciate the breadth of learners within the medical school and easiness to falsely assume one is meeting everyone’s needs. The backgrounds, desires and learning styles can vary drastically from group to group and year to year. Mistakenly applying the methods from one group to another can lead to hurt feelings, misunderstandings and anger. Each group should be assessed as different and teaching methodologies should be adjusted accordingly. Furthermore positive feedback from some does not equate to positive feedback from everyone. I need to be aware of both nonverbal communication and other subtle signs to see determine if teaching methods need to be readjusted.
